Is Gene Editing an Option for My Child’s Rare Disease? How a Custom CRISPR Therapy Saved Baby KJ
When Kyle and Nicole Muldoon's son KJ was born in the summer of 2024, he seemed healthy. Within two days, something was wrong. He was not eating. He could not stay warm. A blood test revealed dangerously high levels of ammonia in his body.
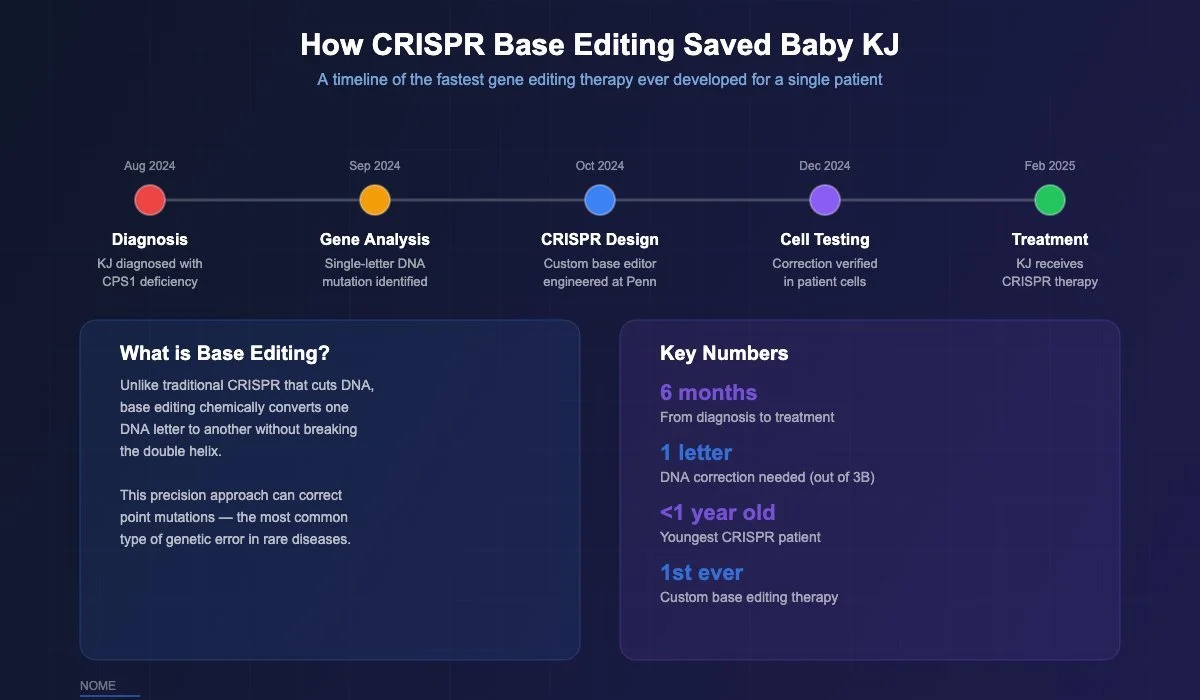
Doctors at Children's Hospital of Philadelphia (CHOP) diagnosed KJ with a condition called CPS1 deficiency. To put it simply: KJ was missing an enzyme his liver needs to break down protein safely. Without that enzyme, a toxic waste product called ammonia builds up in the blood. If it reaches the brain, it can cause permanent damage or death. The condition affects roughly one in a million babies.
KJ's parents were told his only option was a liver transplant, a serious surgery with significant risk for a newborn. But a team of scientists at CHOP and Penn Medicine had been working on something else entirely: a way to fix the root cause of diseases like KJ's by correcting the mistake directly in his DNA.
What happened next changed the future of medicine for rare disease families.
What They Did for Baby KJ
Dr. Rebecca Ahrens-Nicklas, a geneticist at CHOP who specializes in metabolic diseases, and Dr. Kiran Musunuru, a gene editing expert at Penn Medicine, had been preparing for a case exactly like KJ's. For two years, they had been developing a faster way to create custom gene editing treatments for babies born with these kinds of enzyme deficiencies. They had already shown it could work in mice. They were waiting for the right patient.
When KJ was diagnosed in August 2024, they had a crucial insight: KJ's disease was caused by a single-letter mistake in his DNA. Out of 3 billion letters in the human genetic code, one was wrong. That one wrong letter was enough to shut down a critical enzyme and put his life at risk.
But because it was a single-letter mistake, it was also fixable with a technology called base editing, a precise form of the CRISPR gene editing tool. Think of it like a spell-checker for DNA: it finds the one wrong letter and swaps it for the correct one, without cutting or breaking the DNA strand.
The team designed a custom base editor programmed specifically for KJ's mutation. They packaged it inside tiny particles called lipid nanoparticles (essentially microscopic fat bubbles) that would carry the medicine through his bloodstream and into his liver cells, exactly where the broken enzyme was supposed to work.
But before they could treat KJ, they had to make sure it was safe. Dr. Fyodor Urnov at the Innovative Genomics Institute (IGI) at UC Berkeley led the safety analysis, scanning KJ's entire genome to check that the editor would not accidentally change DNA in the wrong place. Jackson Laboratory created a custom mouse with KJ's exact mutation to test the treatment before it reached a human patient. Companies including Aldevron, IDT, Acuitas Therapeutics, and Danaher provided manufacturing and materials support. More than 80 people across the country worked through the fall and winter, including over the holidays.
David Liu, the Harvard scientist who invented base editing, helped optimize the treatment's precision. Ben Kleinstiver at Massachusetts General Hospital contributed to designing the guide that directs the editor to the right spot.
The FDA reviewed their application and approved it in one week.
On February 25, 2025, when KJ was about six months old, he received his first dose through an IV line. He slept through the whole thing.
KJ received two more doses in March and April. There were no serious side effects. His liver enzymes went up briefly (a sign his immune system noticed the treatment) and came back down on their own. He started tolerating more protein in his diet. He needed less medication. When he caught normal childhood viruses that would have been dangerous before, he recovered without any ammonia spikes.
In June 2025, after spending the first ten months of his life in the hospital, KJ went home for the first time. He celebrated his first birthday in August. He took his first steps before Christmas. His weight went from the 7th percentile to the 40th percentile for his age.
What Is Gene Editing and How Is It Different from Other Treatments?
If your child has a rare genetic disease, you have probably heard about several types of treatments: gene therapy, ASO therapy, CRISPR, and drug repurposing. It can be overwhelming to understand the differences. Here is what matters.
Gene editing changes your child's actual DNA. It finds the specific mistake in the genetic code and fixes it. Because DNA is the permanent instruction manual for your cells, this fix can potentially last a lifetime. That is the key difference: gene editing is potentially a one-time treatment.
ASO therapy works on a temporary copy of the DNA called RNA. ASOs correct the instructions your cells are reading right now, but the underlying DNA stays the same. That means ASOs need to be given repeatedly, usually every few weeks or months. ASOs are currently faster and less expensive to develop for individual patients because manufacturing is simpler.
Gene therapy (AAV) delivers a brand new working copy of a broken gene into your child's cells using a harmless virus as a delivery vehicle. It does not fix the original gene; it adds a second, working copy alongside it. Several AAV gene therapies are FDA-approved for rare diseases. A limitation is that the virus can usually only be given once, because the immune system develops antibodies against it.
Drug repurposing uses an existing, already-approved drug for a new purpose. If a drug that was developed for one disease happens to work on the same biological pathway as your child's condition, a doctor can prescribe it right away. This is the fastest option, measured in weeks, but only works when a matching drug exists.
The right option depends entirely on your child's specific mutation, which gene is affected, what the mutation does, and which organ is involved. That is why it matters to evaluate every option in parallel rather than picking one and hoping it works.
Three Types of Gene Editing: Which One Treated Baby KJ?
There are three main gene editing tools available today. They all use CRISPR technology but work in different ways. The easiest way to think about them:
CRISPR-Cas9 is the original and best known. It works like molecular scissors: it cuts the DNA at a specific spot. The cell then repairs the cut, but usually makes small errors that effectively turn off the gene. This is powerful when you want to disable a gene that is making something harmful. The first FDA-approved gene editing drug, Casgevy, uses this approach. It treats sickle cell disease by turning off a gene that suppresses healthy hemoglobin production. In clinical trials, 93.5% of sickle cell patients who received Casgevy were free from severe pain crises for 12 or more months.
Base editing is what treated Baby KJ. Instead of cutting the DNA, it chemically changes one letter to another, like fixing a typo without ripping the page. No cutting, no breaking, no messy repair. Just a clean swap of the wrong letter for the right one. This is ideal for diseases caused by point mutations (single-letter mistakes), which account for a large number of rare genetic diseases. Base editing is currently in clinical trials for sickle cell disease and heart disease, with more than 17 patients treated so far.
Prime editing is the newest and most flexible tool. It can make any single-letter change, plus small insertions and deletions, all without cutting the DNA. Think of it as a find-and-replace function for your genetic code. It is the least tested in patients so far, with the first clinical trial expected to start in 2026, but it has the potential to be the most broadly useful editor in the long run.
How Does the Treatment Get into Your Child's Body?
There are two ways to deliver a gene editing treatment. Which one your child would need depends on where the disease is in the body.
IV infusion (in vivo editing) is what Baby KJ received. The medicine is packaged in tiny fat particles (lipid nanoparticles) and given through an IV, just like a regular infusion. The particles travel through the bloodstream to the liver, enter liver cells, and the editor makes its fix inside the cell. No surgery. No cells removed from the body. No chemotherapy. KJ received three infusions over three months. This approach currently works best for liver diseases, with research underway to reach the brain, eyes, and other organs.
An important advantage of this approach: your child can receive multiple doses. KJ got three. With some other gene therapies that use viruses to deliver treatment, your child's immune system may block a second dose, making re-treatment difficult.
Cell collection and return (ex vivo editing) is what the FDA-approved Casgevy uses for sickle cell disease. Doctors collect blood stem cells from the patient, edit them with CRISPR in a lab, then give them back after chemotherapy clears the bone marrow. This requires weeks in the hospital and the chemo carries its own risks. But for blood diseases, it has produced remarkable results.
What the Innovative Genomics Institute Is Building Next
The team behind Baby KJ's treatment is not stopping at one patient. The Innovative Genomics Institute (IGI) at UC Berkeley, founded by Nobel Prize winner Jennifer Doudna (who co-discovered CRISPR), has been building what they call a "cookbook" for creating these treatments on demand. The idea is to create a repeatable system so that the next baby born with a treatable mutation does not require 80 people working through the holidays to develop a therapy from scratch.
The CHOP and Penn Medicine team is already planning a clinical trial to treat five more patients with correctable mutations in seven different genes that cause urea cycle disorders, the same family of diseases that affected KJ. They are working with the FDA to create a platform approach that could eventually be used for any enzyme deficiency in the liver.
The cost of manufacturing KJ's treatment was approximately $800,000, with significant in-kind support from industry partners. That is expensive, but it is far less than a liver transplant (typically $500,000 or more, plus a lifetime of anti-rejection medication). And as the platform scales and the process becomes standardized, costs are expected to come down significantly.
Is Gene Editing an Option for My Child?
Gene editing may be an option for your child if the disease is caused by a specific, identified genetic mutation (you need a confirmed molecular diagnosis from whole genome sequencing), the mutation is a type that gene editing tools can correct (particularly single-letter point mutations for base editing), the affected organ can be reached by current delivery methods (the liver is well established; brain and eye are in development), and your child still has function to preserve (for progressive diseases, earlier treatment generally means better outcomes).
Gene editing is not the right fit for every rare disease. For some mutations, ASO therapy will be faster. For others, AAV gene therapy may be more appropriate. For diseases with an existing drug that targets the same pathway, drug repurposing may get your child treatment in weeks rather than months or years.
The only way to know which option fits your child is to have the mutation evaluated against every available modality. That is exactly what Nome does.
What Nome Does for Rare Disease Families
Nome Therapeutics provides free genetic analysis for any rare disease family. We evaluate your child's specific mutation and determine which treatments may be realistic options, including gene editing, ASO therapy, gene therapy, clinical trials, and drug repurposing. We do not default to one approach. We evaluate everything in parallel and find the fastest viable path.
Within 1-2 weeks of receiving your genetic diagnosis, our AI platform and PhD scientists deliver a clear, plain-English report explaining what your child's mutation does, which therapies could address it, and what the next steps look like. This evaluation is free, with no cost and no obligation.
For families who want to move forward, we manage the full development process: selecting the right research partners and manufacturers, building the timeline, coordinating the science, and navigating the FDA pathway.
The Baby KJ story proved that personalized gene editing is real, that it can be done in months, and that the infrastructure to scale it is being built right now. For families who have been told "there is nothing we can do," that is no longer true. The question is not whether personalized treatments are possible. It is whether someone is looking at your child's specific mutation with the right tools.
Nome exists to make sure someone is.
Submit your child's genetic diagnosis for a free evaluation at nome.bio.
REFERENCES
1. Ahrens-Nicklas R, Musunuru K, et al. New England Journal of Medicine. 2025. (Baby KJ personalized base editing therapy)
2. Children's Hospital of Philadelphia. "World's First Patient Treated with Personalized CRISPR Gene Editing Therapy." Press release, May 15, 2025.
3. Children's Hospital of Philadelphia. "The Future of Personalized Medicine is Here: KJ's Story." chop.edu.
4. Innovative Genomics Institute. "First Patient Treated with On-Demand CRISPR Therapy." innovativegenomics.org, May 15, 2025.
5. Frangoul H, et al. New England Journal of Medicine. 2021;384:252-260. (Casgevy for sickle cell disease and beta-thalassemia)
6. Anzalone AV, et al. Nature. 2019;576:149-157. (Prime editing)
7. Jonker AH, et al. Nature Reviews Drug Discovery. 2025;24:40-56. (IRDiRC N-of-1 therapy roadmap)
This article is for informational purposes only and does not constitute medical advice.